
 |
| link to article: http://jco.ascopubs.org/content/33/32/3741.full.pdf+html |
Background:
The role of autologous stem cell transplantation (ASCT) in AL amyloidosis is controversial. Single center studies have reported durable, high hematologic responses, organ dysfunction improvement and improved survival. However, a prospective randomized clinical trial by Jaccard et al in 2007 comparing ASCT with oral melphalan and dexamethasone showed inferior survival in the ASCT group. The inferior outcomes were related to high early mortality (EM) of 26% in the transplantation arm. This high early mortality rate could be attributed to patient selection and peritransplant management, the inclusion of patients with severe cardiac involvement, as well as the fact that most transplantation centers in this study were low volume centers. With earlier disease detection and risk stratification of patients with cardiac amyloid and better peritransplantation supportive care, single centers have reported post-transplantation EM rates of <5%. The authors hypothesized that outcomes of autotransplantation in AL amyloidosis have improved over time.
Methods:
Study Design
- Retrospective study utilizing the prospectively generated Center for International Blood and Marrow Transplant Research (CIBMTR) database.
- Transplantation data from over 320 centers around the world
- The data includes disease type, age, sex, date of diagnosis, graft type, conditioning regimen, post-transplantation disease progression, survival, and cause of death
- Registration and research data were collected at pre transplantation, at 100 days post transplantation, at 6 months post transplantation, and annually thereafter until death or last follow up.
Patient Population
- Patients included:
- Patients registered with the CIBMTR in N. America between 1995 and 2012
- Autotransplantation for AL amyloidosis within 24 months of diagnosis
- Data from these patients were analyzed in 3 cohorts based on year of transplantation:
- 1995-2000
- 2001-2006
- 2007-2012
- This dataset was assessed for survival outcomes
- A subgroup of 354 patients with detailed research data who underwent transplantation between 2001-2012 were analyzed for hematologic and organ responses as well as in multivariable analyses. Characteristics of this subset was compared with the registration set to confirm that this was a representative random sample.
Definition of EM:
- Mortality from any cause after transplantation within the defined time window of 30 and 100 days.
Hematologic and renal response and progression
- Defined according to the system proposed at the 10th International Symposium on Amyloidosis in 2004.
- New criteria were proposed to define hematologic response and progression based on free light-chain (FLC) analysis. In this registry, FLC and cardiac biomarkers were only collected after 2008.
- The 2012 hematologic or cardiac response criteria was unable to be applied retrospectively.
- In regards to organ response, only renal responses were reported in this analysis.
Center Effect
- Because there is wide variability in numbers of transplantations performed by centers in this 18-year period, center effect was calculated by using the mean number of transplantations performed for AL amyloidosis per year over 4 years between 2009-2012.
- Maximum likelihood testing was performed using various cut points of transplantations per year.
- It was established that a minimum of 4 transplantations per year was an informative divider for this analysis.
Results:
Patient Characteristics
- Table 1 displays the characteristics of the entire group from 1995-2012 (n=1536). Table 2 shows the subset with detailed data from 2001-2012 (n=354).
- Median age of transplantation was 56 years, with increasing age of transplantation with successive time cohorts.
- Most patients underwent transplantation within 6 months of diagnosis.
- The underlying plasma clone was lambda in 72% of patients.
- M-spike non quantifiable in 42%.
- Distribution of cardiac and renal involvement was similar. Renal without cardiac involvement was most frequent pattern.
- There was no difference in number of organs involved between the 2001-2006 group and 2007-2012 groups, with four or more organs involved in 12% vs 11% patients respectively.
- More patients received treatment before transplantation in the 2007-2012 group (33% vs 13%, p<0.001).
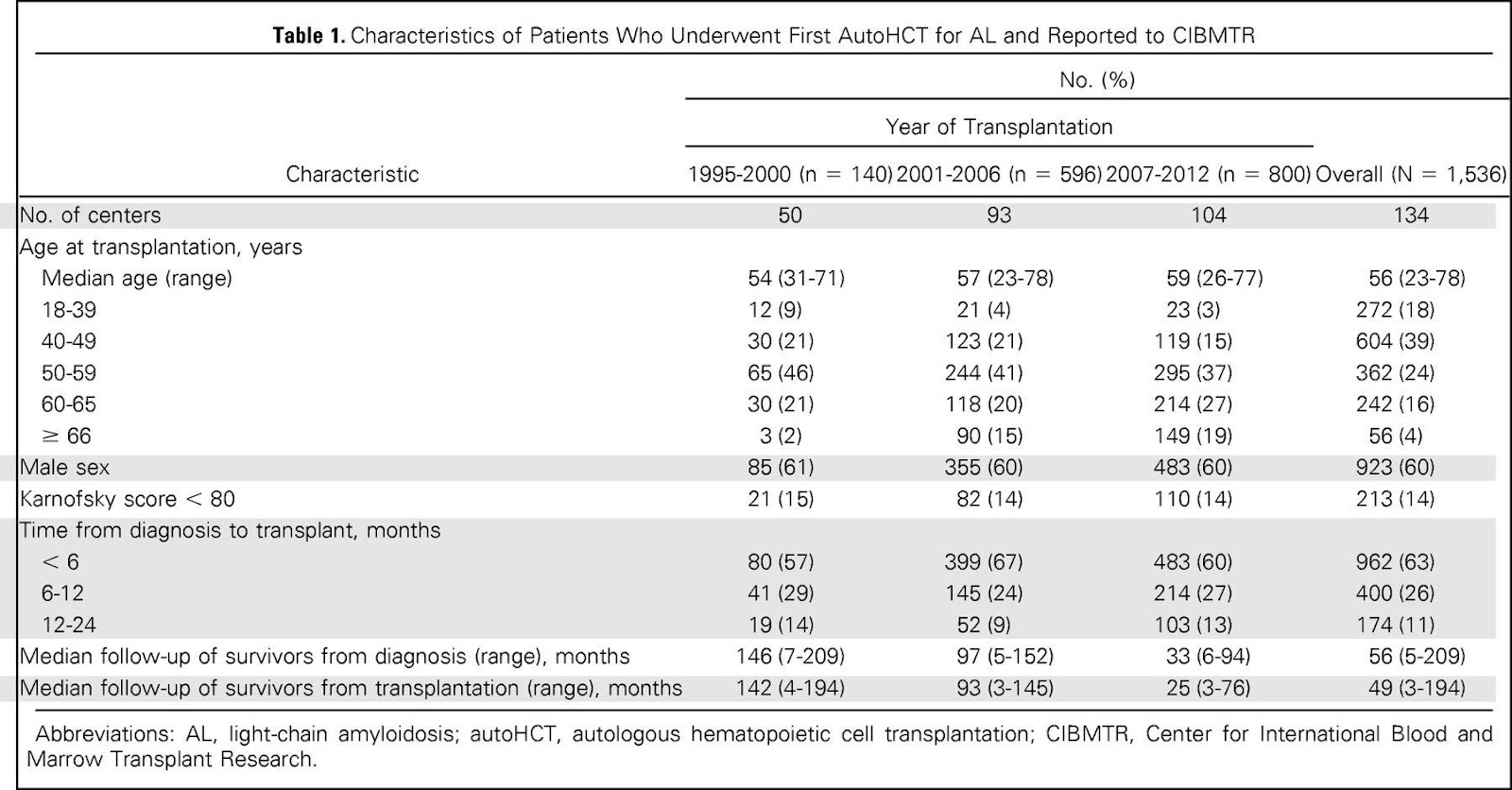 |
| Table 1: Characteristics of 1536 pts who underwent first autoHCT for AL |
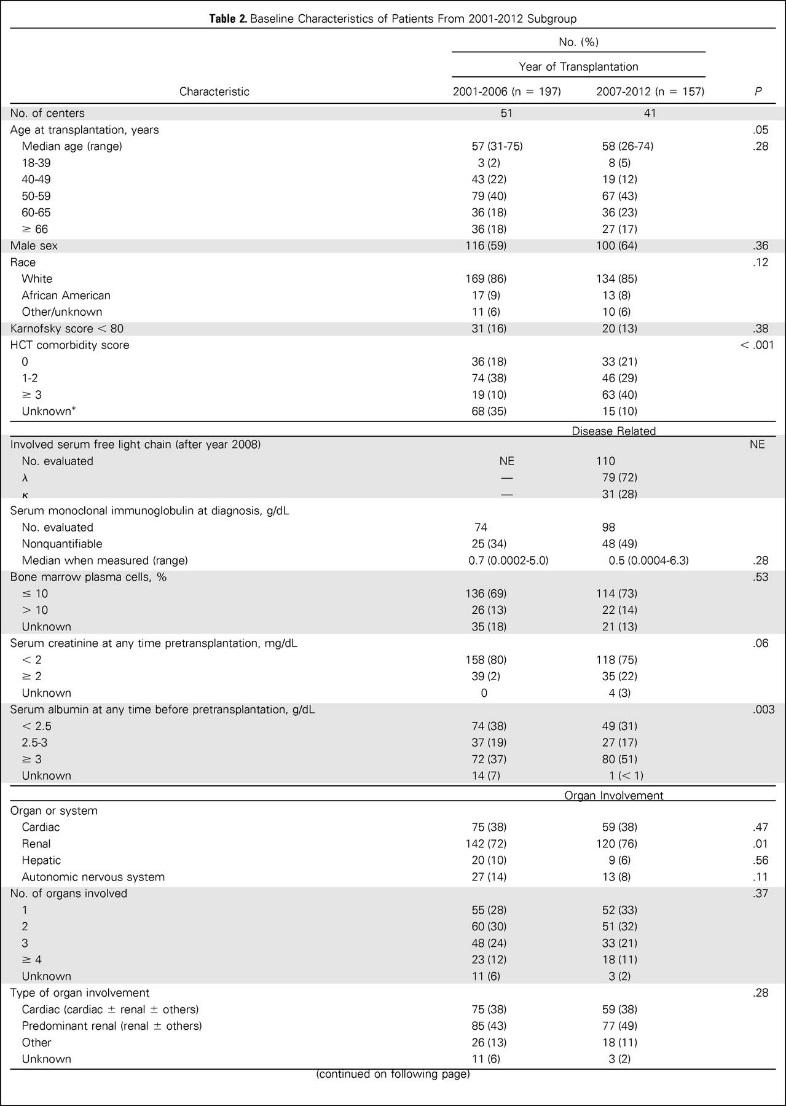 |
| Table 2: baseline characteristics of the 2001-2012 subgroup |
Early Mortality and Causes of Death in all 1536 patients
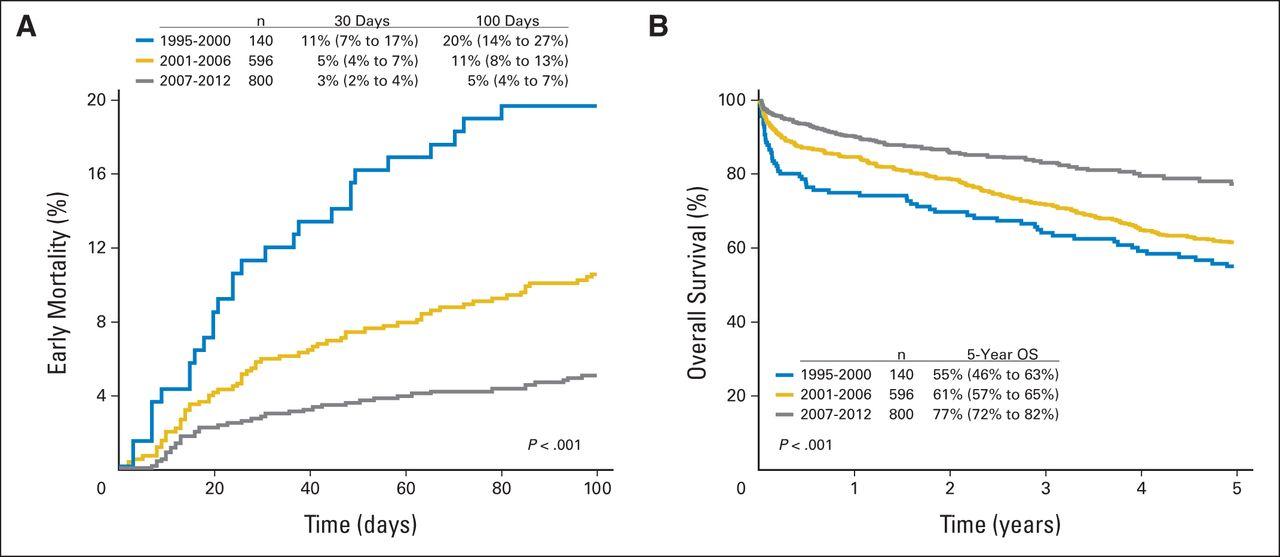
Figure 1A shows EM for all 3 groups.
- Mortality at 30 days
- 1995-2000:11% (95% CI, 7% to 17%)
- 2001-2006: 5% (95% CI, 4% to 7%)
- 2007-2012: 3% (95% CI, 2% to 4%)
- Mortality at 100 days
- 1995-2000: 20% (95% CI, 14% to 27%)
- 2001-2006: 11% (95% CI, 8% to 13%)
- 2007-2012: 5% (95% CI, 4% to 7%)
- Time from diagnosis to transplantation did not affect EM.
- < 6months: 12% (95% CI, 8% to 17%).
- 6-12 months: 5% (95% CI, 1% to 11%).
- 12-24 months: 8% (95% CI, 2% to 18%)
- Causes of death within 100 days
- Amyloid and organ failure (83%)
- Infection (8%)
- Nonengraftment (3%)
- Unknown causes (6%)
OS in 1536 patients
- Median follow up of 56 months
- 1, 3, and 5 year OS increased over time (p<0.001)
- 1995-2000: 75% (95% CI, 65% to 82%), 64% (95% CI, 56% to 72%), 55% (95% CI, 46% to 63%)
- 2001-2006: 85% (95% CI, 81% to 87%), 72% (95% CI, 68% to 75%), 61% (95% CI, 57% to 65%)
- 2007-2012: 90% (95% CI, 88% to 92%), 83% (95% CI, 80% to 86%), 77% (95% CI, 72% to 82%)
- No difference in OS based on time from diagnosis to transplantation (p=0.22)
- < 6months: 73% (95% CI, 67% to 79%)
- 6-12 months: 81% (95% CI, 71% to 89%)
- 12-24 months: 81% (95% CI, 61% to 92%)
- 3 year OS for patients with cardiac amyloidosis improved (p=0.59)
- 2001-2006: 62% (95% CI, 48% to 75%)
- 2007-2012: 67% (95% CI, 52% to 80%)
- 3 year OS for patients with renal and without cardiac amyloidosis improved (p=0.03)
- 2001-2006: 78% (95% CI, 68% to 86%)
- 2007-2012: 89% (95% CI, 82% to 95%)
 |
| Figure 1 |
 |
| Figure 2: Trends in (A) OS for cardiac AL amyloidosis; (B) OS for renal, noncardiac AL; (C) EM based on center experience and (D) time trends in improvement in EM among centers |
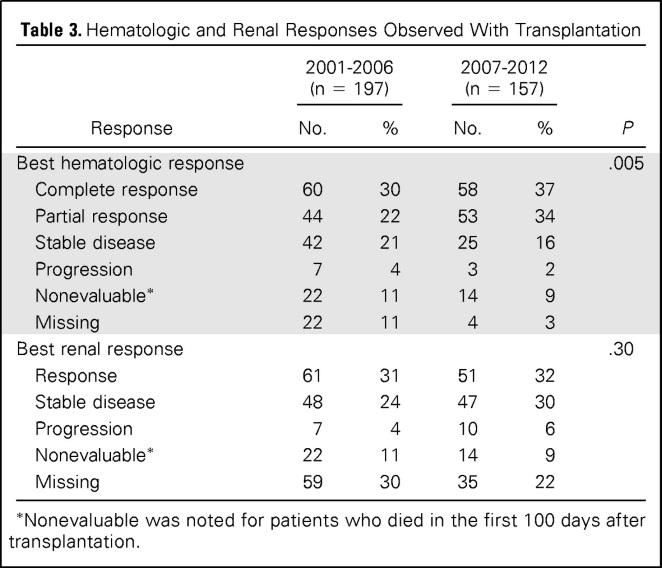
Response rates in subset of 354 patients
- The breakdown of hematologic and renal response rates are shown in Table 3.
Center effects in subset of 354 patients
- 81 low volume centers performed <4 AL transplantations a year
- EM worse in low volume centers (p=0.01)
- 30 day mortality
- Low volume: 5% (95% CI, 3% to 7%)
- High volume: 1% (95% CI, 0.4% to 3%)
- 100 day mortality
- Low volume: 7% (95% CI, 5% to 10%)
- High volume: 3% (95% CI, 2% to 6%)
- No statistically difference found for age, KPS, HCT-CI, cardiac amyloidosis, number of organs involved, melphalan conditioning dosage, pretransplantation chemotherapy between high and low volume centers
- Both high and low volume centers had improvement in EM in 3 time cohorts (p<0.01)
Multivariable analysis in subset of 354 patients
Adjusted analysis show no difference between 2001-2006 cohort and 2007-2012 cohort for EM, PFS, or OS. After 9 months the relapse and/or progression rate was lower in 2007-2012 cohort.
Author's Conclusions:
- Impressive reduction in EM has been achieved in recent years, superior to reported TRM of 24% from the only randomized clinical trial in this setting
- Cardiac amyloid continues to be associated with worse outcomes, with no improvement in outcomes of these patients over time.
- Center experience with AL transplantation important in reducing EM, with high volume centers (defined as having performed 4 or more transplants a year) with better outcomes.
- 5 year survival in most recent cohort is comparable to data from specialized single centers.
Our Comments:
- No cardiac staging information was reported. Although there was no difference in the proportion of patients with cardiac involvement between the cohorts, the lack of information about cardiac biomarkers and staging make it difficult to determine the reasons for improvement in outcome over time.
- Better patient selection could account for the improvement in EM over time, as well as the differences in outcomes between high volume and low volume centers.
- This study looked at a cohort of patients between 1995-2012. However, there was only detailed data reported on organ involvement and hematologic markers in patients treated between 2001-2012.
- Newer approaches to the treatment of advanced cardiac amyloidosis is needed.
- Although this was not a prospective controlled trial, the fact that this study shows EM rates approaching those reported by specialized centers is encouraging.
- A multi-institutional study involving high volume centers comparing transplantation versus non-transplantation therapy (with emergence of newer anti plasma cell therapies) is warranted.
- Role for induction therapy in patients with BM plasmacytosis of >10% should be looked at with respect to OS and EFS
No comments:
Post a Comment